The aetiology and antibiotic management of community-acquired pneumonia in adults in Europe: a literature review
Abstract
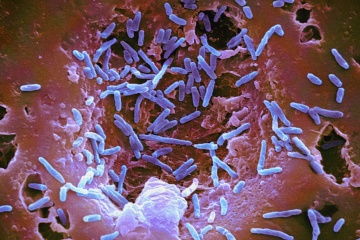
The purpose of this paper was to generate up-to-date information on the aetiology of community-acquired pneumonia (CAP) and its antibiotic management in adults across Europe. Structured searches of PubMed identified information on the aetiology of CAP and its antibiotic management in individuals aged >15 years across Europe. We summarise the data from 33 studies published between January 2005 and July 2012 that reported on the pathogens identified in patients with CAP and antibiotic treatment in patients with CAP. Streptococcus pneumoniae was the most commonly isolated pathogen in patients with CAP and was identified in 12.0–85.0 % of patients. Other frequently identified pathogens found to cause CAP were Haemophilus influenzae, Gram-negative enteric bacilli, respiratory viruses and Mycoplasma pneumoniae. We found several age-related trends: S. pneumoniae, H. influenzae and respiratory viruses were more frequent in elderly patients aged ≥65 years, whereas M. pneumoniae was more frequent in those aged <65 years. Antibiotic monotherapy was more frequent than combination therapy, and beta-lactams were the most commonly prescribed antibiotics. Hospitalised patients were more likely than outpatients to receive combination antibiotic therapy. Limited data on antibiotic resistance were available in the studies. Penicillin resistance of S. pneumoniae was reported in 8.4–20.7 % of isolates and erythromycin resistance was reported in 14.7–17.1 % of isolates. Understanding the aetiology of CAP and the changing pattern of antibiotic resistance in Europe, together with an increased awareness of the risk factors for CAP, will help clinicians to identify those patients most at risk of developing CAP and provide guidance on the most appropriate treatment.
 The bronchial microbiome in severe COPD during stability and exacerbation in patients chronically colonised by Pseudomonas aeruginosa (PA), has not been defined. Our objective was to determine the characteristics of the bronchial microbiome of severe COPD patients colonised and not colonised by P. aeruginosa and its changes during exacerbation.
The bronchial microbiome in severe COPD during stability and exacerbation in patients chronically colonised by Pseudomonas aeruginosa (PA), has not been defined. Our objective was to determine the characteristics of the bronchial microbiome of severe COPD patients colonised and not colonised by P. aeruginosa and its changes during exacerbation. Several reports have shown that segmentectomy is superior to lobectomy for preservation of postoperative pulmonary function. The purpose of this study was to characterize the relationship between pulmonary function and the volume of the resected lung in patients undergoing segmentectomy or lobectomy.
Several reports have shown that segmentectomy is superior to lobectomy for preservation of postoperative pulmonary function. The purpose of this study was to characterize the relationship between pulmonary function and the volume of the resected lung in patients undergoing segmentectomy or lobectomy.